Pesquisa
US Quiz of the Month – dezembro 2025
Case Report
A 66-year-old male with a history of dyslipidemia, hypertension, and obstructive sleep apnea was referred for surgical evaluation after an incidental finding on abdominal computed tomography (CT). The contrast-enhanced CT revealed a 19 mm hypervascular, exophytic lesion in the second portion of the duodenum (D2). The patient was asymptomatic, denying abdominal pain, weight loss, gastrointestinal bleeding, or jaundice. Physical examination and laboratory workup (complete blood count, liver enzymes, bilirubin and tumor markers) were unremarkable.
To further characterize the lesion, endoscopic ultrasound (EUS) was performed. Surprisingly, EUS failed to identify a clear duodenal wall bulge. Instead, in the periduodenal area, an extramural, 20 mm, well-circumscribed, heterogeneous lesion was noted, exhibiting internal vascularization on Doppler study and small anechoic areas. No adjacent peritoneal effusion or lymph nodes were found. Due to diagnostic uncertainty and the suspicion of a duodenal neoplasm, surgical resection was proposed after a multidisciplinary discussion.
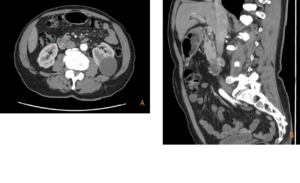
Figure 1: Transverse (A) and sagittal (B) CT images showing a 19 mm hypervascular lesion in the D2
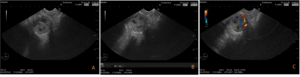
Figure 2: EUS findings: in D2, an extramural rounded 20 mm heterogeneous lesion (A e B), exhibiting vascularization on Doppler study (C) and internal anechoic areas (A), with no duodenal wall bulge. FNB was not performed according to multidisciplinary decision.
What is the most likely diagnosis?
Discussion
Surgical laparotomy exploration revealed that the lesion was not duodenal in origin. Instead, a vascular mass was identified arising from the right gonadal vein, with a feeding vessel originating from the anterior surface of the inferior vena cava and focal thrombosis at its insertion. The right gonadal vein’s anatomical proximity to D2 explains why vascular anomalies in this region can mimic duodenal neoplastic lesions on cross-sectional imaging.
Anastomosing hemangioma (AH) is a rare, benign vascular variant primarily found in the genitourinary tract, especially the kidneys and retroperitoneum. It is typically discovered incidentally. The primary clinical challenge lies in its nonspecific imaging features, which often resemble malignant tumors like angiosarcoma. This overlap can lead to diagnostic uncertainty and potentially unnecessary surgical interventions. Histologically, AH consists of anastomosing capillary-sized channels lined by “hobnail” endothelial cells without cytological atypia. Immunohistochemistry is crucial for confirmation, typically showing positivity for CD31, CD34, and ERG, and a low Ki-67 index (<5%), distinguishing it from more aggressive vascular malignancies.
This case underscores the importance of including vascular anomalies in the differential diagnosis of hypervascular lesions adjacent to the duodenum and highlights the role of EUS in identifying the extramural origin of such masses.
References
1.Montgomery E, Epstein JI. Anastomosing hemangioma of the genitourinary tract: a lesion mimicking angiosarcoma. Am J Surg Pathol. 2009 Sep;33(9):1364-9. doi:10.1097/PAS.0b013e3181ad30a7.
2.Hoxhaj I, Piccino M, Grossi U, Maffeis V, Beleù A, Baciorri F, Morana G, Zanatta P, Zanus G. Systematic Review and Case Report of a Left Gonadal Vein Anastomosing Hemangioma. J Clin Med. 2025;14(9):3108. doi:10.3390/jcm14093108
3.Barat M, Dohan A, Dautry R, Barral M, Boudiaf M, Hoeffel C, Soyer P. Mass-forming lesions of the duodenum: a pictorial review. Diagn Interv Imaging. 2017;98(10):663-675. doi:10.1016/j.diii.2017.01.004
4.Laih CY, Hsieh PF, Chen GH, Chang H, Lin WC, Lai CM, Chang CH. A retroperitoneal cavernous hemangioma arising from the gonadal vein: a case report. Medicine (Baltimore). 2020;99: e22325. doi:10.1097/MD.0000000000022325
Authors
Ana Catarina Gomes1, Ricardo Martins2, Rui Caetano Oliveira3, Alexandra Fernandes1, Helena Vasconcelos1
1 – Serviço de Gastrenterologia, Unidade Local de Saúde da Região de Leiria
2 – Serviço de Cirurgia Geral, Unidade Local de Saúde da Região de Leiria
3 – Centro de Anatomia Patológica Germano de Sousa