Pesquisa
US Quiz of the Month – May 2020
CASE REPORT
A 57-year-old asymptomatic male, with a medical history of nephrectomy due to renal cell carcinoma, was referred to our Gastroenterology Department following incidental detection on annual follow-up computed tomography (CT) of a gastric mass measuring 35mm x 28mm, located on the posterior wall of the transition body-antrum. The lesion was well demarcated and round shaped, with central calcification, dense enhancement and a small area of central necrosis (Fig. 1). There was no evidence of local recurrence of the renal cell carcinoma, metastatic disease, adenopathy, ascites or peritoneal implants.

Figure 1. Abdominal and pelvic CT (axial view): gastric mass located on the posterior wall of the stomach
Endoscopic ultrasonography (EUS) documented a subepithelial lesion on the posterior wall of the stomach, body-antrum transition, measuring 36mm x 29m, heterogeneously hypoechoic, hypervascular, with irregular but well-defined limits and central calcification, arising from the 4th layer, without invasion of adjacent layers (Fig. 2 and 3). EUS-FNA using a 22-gauge needle was performed.
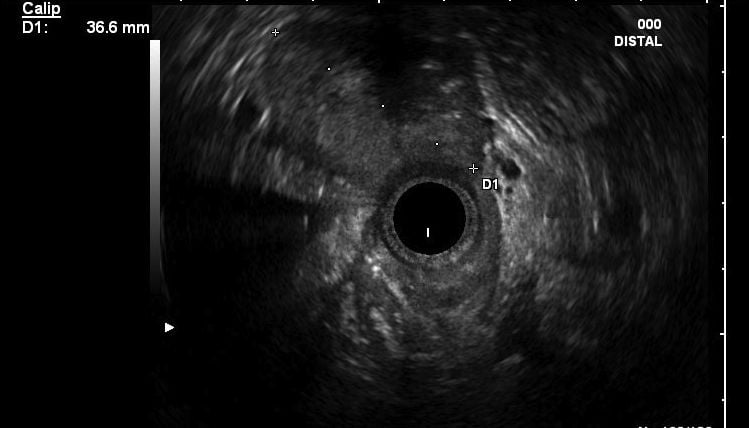
Figure 2. EUS: Subepithelial lesion of the posterior wall of the stomach, heterogeneously hypoechoic and with well defined limits.
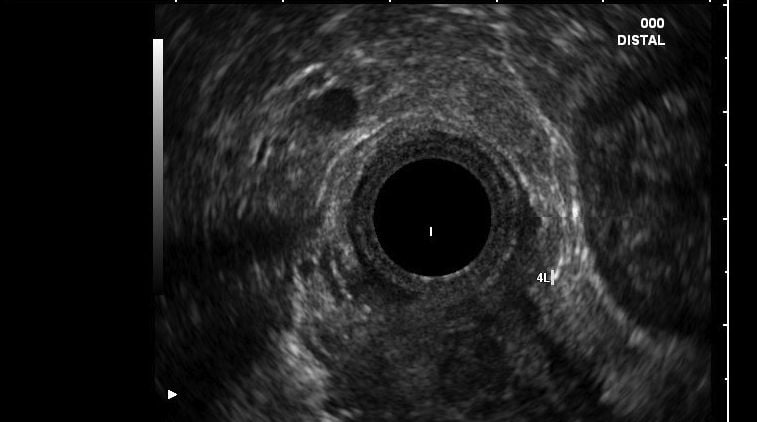
Figure 3. EUS: Subepithelial lesion of the posterior wall of the stomach arising from the 4th layer.
WHAT IS THE MOST LIKELY DIAGNOSIS?
DISCUSSION
The EUS-FNA specimen revealed some smooth muscular cells and a proliferation of uniform cells with a rounded and regular shape, round nucleus, clear cytoplasm and a high nucleus-cytoplasm ratio and perivascular distribution. The cells did not have nuclear atypia or mitotic activity. Immunohistochemical staining was positive for smooth muscle actin, type IV collagen and cytokeratin AE1/AE3. The pathologic diagnosis of gastric glomus tumour was made. After multidisciplinary decision, the tumour was completely removed through a submucosal wedge gastric resection. The patient did not receive any adjuvant therapy because the tumour did not show signs of malignancy. Two years after surgery, the patient remains asymptomatic and disease free.
Glomus tumour is a rare mesenchymal neoplasm originating from the normal glomus body, a specialized arteriovenous anastomosis responsible for thermoregulation. It usually occurs in the peripheral soft tissue of extremities, as the subungual region of the finger, and represents 1.6% of all soft tissue tumours. Despite its rarity, glomus tumours have been reported in almost every location, including the stomach. Gastric glomus tumour usually presents as a subepithelial lesion arising from the submucosa or muscularis propria layers. It accounts for 1% of all gastric subepithelial lesions. It is usually an incidental finding but it can present with upper digestive bleeding. The recommended standard treatment is surgical resection. The prognosis is good because of the low risk of relapse and rare malignant transformation, but prolonged follow-up is recommended.
REFERENCES
- Kang G, Park HJ, Kim JY, et al. Glomus tumor of the stomach: a clinicopathologic analysis of 10 cases and review of the literature. Gut Liver. 2012;6(1):52–57.
- Handa Y, Kano M, Kaneko M, Hirabayashi N. Gastric Glomus Tumor: A Rare Cause of Upper Gastrointestinal Bleeding. Case Rep Surg. 2015;2015:193684.
- Papadelis A, Brooks CJ, Albaran RG. Gastric glomus tumor. J Surg Case Rep. 2016;2016(11):rjw183.
AUTHORS
Borges VP1, Loureiro RV1, Santos S1, Carvalho D1, Ramos G1
- Gastroenterology Department, Centro Hospitalar Universitário de Lisboa Central E.P.E., Lisbon, Portugal