Pesquisa
US Quiz of the Month – November 2021
CASE REPORT
The authors present the case of a 68-year-old male patient with a history of smoking and chronic cough. A thoracic CT scan was performed and revealed a mass with mediastinal invasion in the left upper lobe and a nodule in the right lung. An abdominal CT scan documented a mass of 40×35 mm in the transition between the body and tail of the pancreatic gland, as well as a nodule in the right adrenal gland, three small liver nodules and a nodule in the right kidney.
An endoscopic ultrasonography (EUS) was performed and identified a heterogeneous, hypoechoic solid lesion, with a clearly defined irregular borders, measuring 17.8 x 20.5 mm. Fine needle biopsy (FNB) was performed (Acquire 22 G, Boston Scientific).
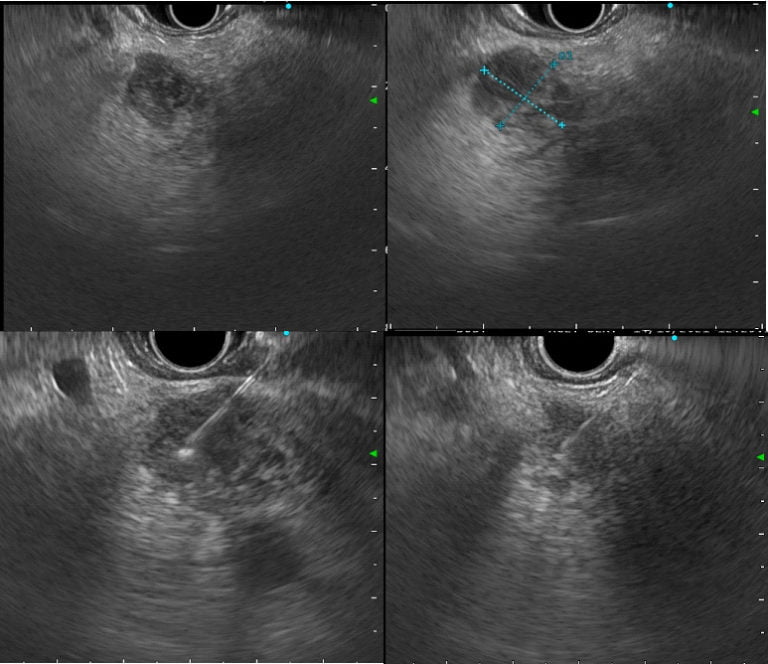
Figure 1. EUS (transgastric view): A heterogeneous hypoechoic solid lesion, with a clearly defined irregular borders, measuring 17.8 x 20.5 mm, located between the body and tail of the pancreatic gland. FNB was performed.
WHAT IS THE MOST LIKELY DIAGNOSIS?
DISCUSSION
These findings were compatible with pancreatic metastasis of lung cancer. Histopathological analysis revealed small cell high grade neuroendocrine carcinoma, positive for cytokeratin AE1/AE3, CAM 5.2, TTF1, CD56 and synaptophysin and negative for p40 and chromogranin; Ki67 antibody was positive in 40-50% of neoplastic cells. Positivity for TTF1 suggested it was a primary tumor of the lung – small cell lung carcinoma. A final diagnosis of metastatic small cell lung carcinoma was made.
Metastatic tumors of the pancreas are responsible for 1-2% of all pancreatic solid lesions [1]. On EUS they show clearly delimitated borders, and are usually heterogeneous and hypoechoic [1,2]. Renal cell carcinoma is the most common metastatic tumor of the pancreas [2,3]. Other secondary tumors of the pancreas include lung, breast, melanoma, colon, stomach and lymphoma [2,3]. Lung cancer comprises around 18,7% of pancreatic metastatic tumors and small cell lung cancer (SCLC) is the most common histological type [3]. Only 2-3% of lung cancer patients present pancreatic metastases [3]. Most patients have no symptoms related to the pancreatic metastasis, but it can directly invade pancreatic ductal epithelium and may clinically mimic primary pancreatic adenocarcinoma [3]. Pancreatic metastasis generally constitutes a late manifestation of widespread disseminated metastasis in cancer patients, and in SCLC it indicates visceral widespread and it is of ominous prognostic importance [3].
SCLC constitutes 15% of all lung cancers [4]. It is an aggressive neuroendocrine carcinoma with high rate of metastasis and the majority of patients (70%) present with extensive disease [4]. Histologically, SCLC can be further classified into small cell carcinoma and combined subtype [4]. Immunohistochemical findings are positive for CD56 (neural cell adhesion molecule, NCAM), which is the most sensitive for the diagnosis of SCLC [5]. Chromogranin and synaptophysin are true markers of neuroendocrine differentiation and are typical of carcinoid tumors, but may be positive in SCLC [5]. Ki67 is positive in at least 40 to 50% of cells [5]. Positivity for TTF1 is much more frequent in SCLC (90%) but it may also be present in pancreatic neuroendocrine tumors (7%), therefore it cannot be used as the sole criteria for distinguishing lung from pancreatic origin [5,6].
REFERENCES
- Yamashita Y. and Kitano M., Endoscopic ultrasonography for pancreatic solid lesions, Journal of Medical Ultrasonics, 2020 47(3):377-387.
- Cortez N., Berzosa M., Mahfouz M., et al, Diagnosis and Treatment of Metastatic Disease to the Pancreas, Journal of Laparoendoscopic & Advanced Surgical Techniques, 2020 30(9):1008-1012.
- Gonlugur U., Mirici A. and Karaayvaz M., Pancreatic involvement in small cell lung cancer, Radiology and Oncology, 2014 48(1):11-9.
- Wang Y., Zou S., Zhao Z., et al, New insights into small‐cell lung cancer development and therapy, Cell Biology International, 2020 44:1564–1576.
- Yatabe Y., Dacic S., Borczuk A.C. et al, Best Practices Recommendations for Diagnostic Immunohistochemistry in Lung Cancer, Thoracic Oncology, 2019 14(3):377–407.
- Wang J., Trivedi P. and El-Bahrawy M., Positivity rate of TTF-1 on immunohistochemistry in pancreatic neuroendocrine tumors, Pathology International, 2016 66(12):708-709.
AUTHORS
Diogo Bernardo Moura1, Nuno Nunes1, Carolina Chálim Rebelo1, Margarida Flor de Lima1, Maria Antónia Duarte.
- Gastroenterology Department, Hospital do Divino Espírito Santo de Ponta Delgada, Ponta Delgada, Portugal.