Pesquisa
US Quiz of the Month – October 2020
CASE REPORT
A 31-year-old asymptomatic female was referred to our department following the incidental detection on abdominal ultrasound of a 54x40mm pancreatic echogenic mass (Fig. 1).
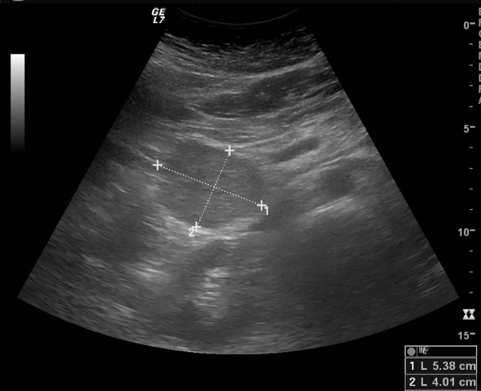
Figure 1 – Abdominal ultrasound: echogenic pancreatic mass measuring 54x40mm.
Abdominal magnetic resonance (MRI) revealed a 54-mm lesion in the uncinated process of the pancreas, well-defined, heterogeneous, with internal septa and solid content, presenting with high signal intensity in T2-weighted images, low signal intensity in T1-weighted images and progressive enhancement; no dilation of the main pancreatic duct nor hepatic lesions were visible (Fig. 2).

Figure 2 – Abdominal MRI (axial view): well-defined heterogeneous lesion, with high signal intensity in T2-weighted images, located in the uncinated process of the pancreas.
Endoscopic ultrasonography (EUS) documented an exophytic heterogeneous 48-mm mass, with solid hypoechogenic component and infracentimetric cystic areas, in the uncinated process of the pancreas, adjacent to the mesenteric vessels (Fig. 3). There were no parenchymal calcifications or atrophy, nor dilation of the main pancreatic duct, and no adenopathy was visible. EUS-fine needle biopsy (FNB) was performed with a 22-gauge needle (Fig. 4) and revealed a neoplasia with a microacinar and solid architecture and well-diferentiated epithelial cells arranged around fibrovascular stalks.

Figure 3 – EUS (D2): exophytic heterogeneous 48-mm mass, with solid hypoechogenic component and infracentimetric cystic areas, located in the uncinate process of the pancreas.
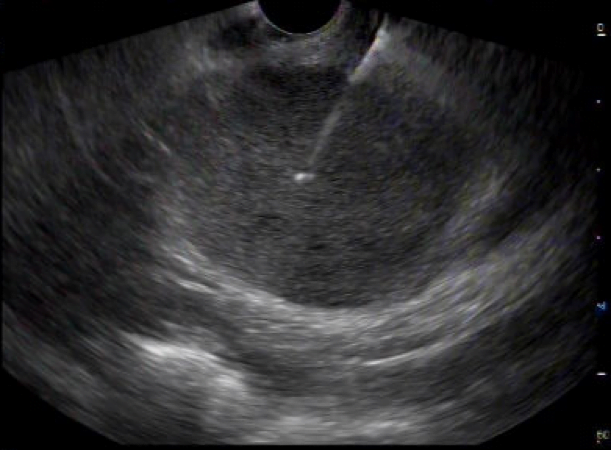
Figure 4 – EUS (D2): EUS-FNB of the pancreatic lesion (22-gauge needle).
WHAT IS THE MOST LIKELY DIAGNOSIS?
DISCUSSION
Patient underwent a pancreaticoduodenectomy and histopathological examination revealed a solid pseudopapillary tumor (SPT) of the pancreas (beta-catenin, CD10 and progesterone receptor positivity).
SPTs of the pancreas are an uncommon entity representing 2-3% of pancreatic neoplasms, primarily affecting young females (average age 30 years)1,2. It has nonspecific clinical presentations and a considerable percentage of patients are asymptomatic1. SPT can be detected by ultrasonography, computerized tomography or MRI, typically presenting as a well-circumscribed mass consisting of solid and cystic components, mostly located in the pancreatic body and tail1,3. Most SPTs exhibit a low malignant potential; complete surgical excision is the treatment of choice, and its prognosis is excellent even for patients requiring extended en bloc resections or concomitant metastasectomy2.
REFERENCES
- Dinarvand P, Lai J. Solid pseudopapillary neoplasm of the pancreas a rare entity with unique features. Arch Pathol Lab Med 2017; 141:990-995.
- Stark A, Donahue T, Reber H, et al. Pancreatic Cyst Disease: a review. JAMA 2016;315:1882-1893.
- Hansen C, Kristensen T, Federspiel, et al. Solid pseudopapillary neoplasm of the pancreas: Clinical-pathological features and management, a single center experience. Rare tumors 2019; 11:1-8.
AUTHORS
Catarina Felix1; Joana Carmo1; Cristina Chagas1.
- Gastroenterology Department, Centro Hospitalar de Lisboa Ocidental, Lisbon, Portugal.