Pesquisa
US Quiz of the Month – julho 2025
Case Report
A 68-year-old male with no previous history of gastrointestinal disease presented with complaints of pyrosis and dyspepsia. An esophagogastroduodenoscopy revealed a subepithelial bulging in the periampullary region of the second part of the duodenum. Subsequent abdominal CT showed a 15 mm, non-enhancing cystic lesion at the level of the ampulla of Vater.
An endoscopic ultrasound (EUS) was performed for further characterization. It showed a normal biliary tree, pancreas, main pancreatic duct, and mesenteric vessels. A well-defined, anechoic cystic lesion was identified in the intra-duodenal segment of the common bile duct, without a muscular wall lining. No mural nodules or suspicious features were observed.
What is the most likely diagnosis?
Discussion
Choledochoceles, classified as Todani type III cysts, are rare cystic dilations of the distal common bile duct that protrude into the duodenal lumen (Todani et al., 1977). They account for less than 5% of choledochal cysts and are often diagnosed incidentally (Singham et al., 2007). Clinical manifestations, when present, may include abdominal pain, acute pancreatitis, or biliary obstruction (Soares et al., 2014).
In this case, the cyst was an incidental endoscopic finding during workup for unrelated upper gastrointestinal symptoms. Further characterization with EUS revealed a well-defined, anechoic cystic lesion arising from the distal common bile duct, lined by duodenal mucosa and lacking a muscular layer, which were sufficient diagnostic features. Duodenal duplication cysts may present similarly but are typically covered both inside and out with duodenal mucosa containing a distinct layer of smooth muscle, which was absent here (Dipasquale et al., 2020). Pancreatic pseudocysts are generally associated with prior pancreatitis and may communicate with the main pancreatic duct, features that were not present in this case. Mucinous cystic neoplasm are larger lesions with complex features predominantly found in middle-aged women and usually located in the pancreatic body or tail(Nilsson et al., 2016). Intramural hematomas tend to follow trauma or anticoagulation therapy and generally spontaneously resolve after a few weeks.
Choledochoceles are considered to carry a lower risk of malignant transformation compared to other types of biliary cysts. When symptoms such as abdominal pain or obstructive jaundice are present, management may include endoscopic sphincterotomy or surgical resection (Lobeck et al., 2017).
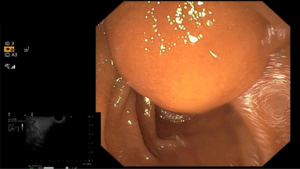
Figure 1. Endoscopic image showing subepithelial bulging in the periampullary region of the second part of the duodenum.
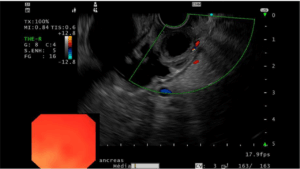
Figure 2. EUS image showing a well-defined, anechoic cystic lesion in the intra-duodenal portion of the common bile duct.
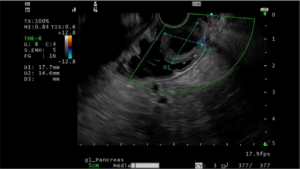
Figure 3. EUS image displaying size measurements of the choledochocele.
References
Dipasquale, V. et al. (2020) ‘Duodenal Duplication Cysts in Children: Clinical Features and Current Treatment Choices’, Biomedicine Hub, 5(2), pp. 1–13. Available at: https://doi.org/10.1159/000508489.
Lobeck, I.N. et al. (2017) ‘The presentation and management of choledochocele (type III choledochal cyst): A 40-year systematic review of the literature’, Journal of Pediatric Surgery, 52(4), pp. 644–649. Available at: https://doi.org/10.1016/j.jpedsurg.2016.10.008.
Nilsson, L.N. et al. (2016) ‘Nature and management of pancreatic mucinous cystic neoplasm (MCN): A systematic review of the literature’, Pancreatology, 16(6), pp. 1028–1036. Available at: https://doi.org/10.1016/j.pan.2016.09.011.
Singham, J. et al. (2007) ‘Choledochal cysts: analysis of disease pattern and optimal treatment in adult and paediatric patients’, HPB : The Official Journal of the International Hepato Pancreato Biliary Association, 9(5), pp. 383–387. Available at: https://doi.org/10.1080/13651820701646198.
Soares, K.C. et al. (2014) ‘Choledochal cysts: presentation, clinical differentiation, and management’, Journal of the American College of Surgeons, 219(6), pp. 1167–1180. Available at: https://doi.org/10.1016/j.jamcollsurg.2014.04.023.
Todani, T. et al. (1977) ‘Congenital bile duct cysts: Classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst’, The American Journal of Surgery, 134(2), pp. 263–269. Available at: https://doi.org/10.1016/0002-9610(77)90359-2.
Authors
João Carlos Gonçalves1,2,3, Pedro Campelo1,2,3, Francisca Dias de Castro1,2,3, Joana Magalhães1,2,3, José Cotter1,2,3
1 – Gastroenterology Department, Hospital da Senhora da Oliveira, Guimarães, Portugal.
2 – Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal.
3 – ICVS/3B’s – PT Government Associate Laboratory, Braga/Guimarães, Portugal.