Pesquisa
US Quiz of the Month – Julho 2024
Case Report
A 38-year-old male, originally from Uzbekistan, living in Portugal for the last 8 years, working as a mechanic, was referred to the Gastroenterology Consultation for liver nodules. An abdominal ultrasound was performed at our institution, and 3 nodular lesions were identified with the images presented below (Fig. 1-3).

Fig. 1 – Nodular lesion in segment VIII with 63x61mm, with hypoechoic and hyperechoic signal, whose pattern resembles a “ball of wool”.

Fig. 2 – Nodular lesion in segment VI with 60x60mm, with hypoechoic and hyperechoic signal, whose pattern resembles a “ball of wool”.
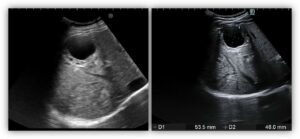
Fig. 3 – Nodular lesion in segment V with 54x46mm, with multivesicular “honeycomb” appearance with septa.
Which is the most appropriate approach in this patient?
Discussion
Hydatid disease, or echinococcosis, is a zoonosis most frequently caused by Echinococcus granulosus, which can affect the liver, lungs, central nervous system and other organs (1-3). Clinical manifestations depend on the organ involved and the viability of the cyst contents, but most patients are asymptomatic and hydatic cysts are found incidentally on routine imaging (2, 3). Complications of this disease include allergic reactions, septic shock due to bacterial translocation, fistula, rupture or symptoms of expanding mass with pressure on adjacent structures (1, 2).
The diagnosis relies on serology and US: serology of Echinococcus granulosus by ELISA is positive in 70% of cases, and the WHO classification system (Fig. 4) contains six categories, based on the imaging appearance, which depends on the stage of the disease (2, 3). The cystic echinococcosis (CE) stages 1 and 2 correspond to active stages, with CE 1 appearing as a uniform anechoic cyst with internal echoes and CE 2 having a multivesicular “honeycomb” appearance with septa (2). The stage 3 is a transitional stage, with CE3A having a unique cyst with detached laminated membranes described as the “water lily sign” and CE3B having daughter cysts within a solid matrix (2). The CE stages 4 and 5 correspond to an inactive and degenerative stage, where there is a hypoechoic and hyperechoic signal, whose pattern resembles a “ball of wool” and there are no more daughter cysts (2).

Fig. 4 – The WHO classification of hydatid cysts, based on the imaging appearance (2).
In patients with active cysts, treatment is indicated, based on the administration of mebendazole or albendazole, in association with surgical resection or a percutaneous treatment guided by ultrasound, known as PAIR (Puncture, Aspiration, Installation of scolicidal agent and Reaspiration), mainly in cysts with more than 50 mm of diameter (1, 2). Inactive cysts in asymptomatic patients do not require treatment (2).
References
- Marrero JA, Ahn J, Rajender Reddy K. ACG clinical guideline: the diagnosis and management of focal liver lesions. Am J Gastroenterol. 2014;109(9):1328-47; quiz 48.
- Wen H, Vuitton L, Tuxun T, Li J, Vuitton DA, Zhang W, et al. Echinococcosis: Advances in the 21st Century. Clin Microbiol Rev. 2019;32(2).
- Chenin M, Paisant A, Lebigot J, Bazeries P, Debbi K, Ronot M, et al. Cystic liver lesions: a pictorial review. Insights Imaging. 2022;13(1):116.
Authors
Ana Isabel Ferreira 1,2,3, Sofia Xavier 1,2,3, Sílvia Leite 1,2,3, Carla Marinho 1,2,3, José Cotter 1,2,3.
- Gastroenterology Department, Unidade Local de Saúde do Alto Ave, Guimarães, Portugal.
- Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal.
- ICVS/3B’s, PT Government Associate Laboratory, Guimarães/Braga, Portugal.