Pesquisa
US Quiz of the Month – outubro 2025
Case Report
The authors present the case of a 63-year-old woman with a past medical history of arterial hypertension, dyslipidemia and type 2 diabetes mellitus, who presented to the gastroenterology office for a screening colonoscopy due to a family history of colon cancer. The colonoscopy showed a subepithelial lesion of about 30 mm in diameter, with normal overlying mucosa, in the left lateral wall of the rectum, approximately at 9 cm from the superior anal margin (figure 1). No other lesions were found in the other colon segments.
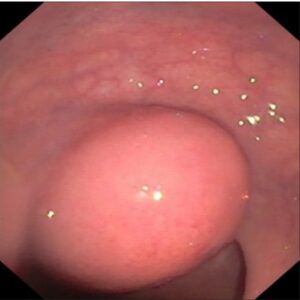
Figure 1: Subepithelial lesion, located at the left lateral wall of the rectum.
Endoscopic ultrasound confirmed the presence of a well circumscribed homogeneous hypoechoic lesion, with well-defined borders, measuring approximately 34 x 30 mm, arising from the muscular layer. Fine-needle biopsy using a 22-gauge needle was performed (figure 2).
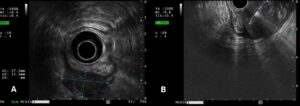
Figure 2: (A) EUS shows a homogeneous hypoechoic lesion, with well-defined borders (34×30 mm), arising from the muscular layer; (B) Tissue sampling was performed using 22-gauge fine needle biopsy (FNB).
What is the most likely diagnosis?
The pathological analysis revealed the presence of compact spindle cells arranged in short bundles and forming interlacing fascicles with nuclear palisading in verocay bodies. Immunohistochemical staining further supported the diagnosis, showing strong positivity for S100 and SOX10, with negative results for CD34, CD117, and SMA. The histological and immunohistochemical features were compatible with a diagnosis of schwannoma.
Discussion
Schwannomas are slow-growing and benign nerve sheath tumors arising from schwann cells, with low risk of malignant transformation. Schwannomas of the gastrointestinal tract are uncommon mesenchymal neoplasms, comprising approximately 2–6% of all such tumors, with those arising in the rectum being exceptionally rare. 1,2
Rectal schwannomas may cause symptoms such as obstruction, bleeding, and tenesmus, but most cases remain asymptomatic. 1 They are most frequently discovered incidentally during endoscopic or imaging studies, where they typically appear as well-circumscribed subepithelial lesions originating from the Auerbach’s (myenteric) or Meissner’s (submucosal) nerve plexuses, in the muscularis propria (4th layer) and in submucosal (3rd layer), respectively. 3,4
Given the benign nature of gastrointestinal schwannomas, asymptomatic patients do not appear to require further surveillance or intervention if the diagnosis is clear, whereas complete surgical or endoscopic excision with negative margins is the mainstay of treatment for symptomatic patients.5,6
Although extremely rare, schwannoma should be included in the differential diagnosis of rectal subepithelial lesions, with endoscopic ultrasonography representing a pivotal tool for diagnostic assessment.
References
- Bohlok A, El Khoury M, Bormans A, et al. Schwannoma of the colon and rectum: a systematic literature review. World J Surg Oncol. 2018;16(1):125.
- Bugiantella W, Rondelli F, Mariani L, Peppoloni L, Cristallini E, Mariani E. Schwannoma of the colon: A case report. Oncol Lett. 2014;8(6):2511-2512.
- Sakamoto H, Kitano M, Kudo M. Diagnosis of subepithelial tumors in the upper gastrointestinal tract by endoscopic ultrasonography. World J Radiol. 2010;2(8):289-297.
- Barbeiro S, Martins C, Gonçalves C, et al. Schwannoma-A Rare Subepithelial Lesion of the Colon. GE Port J Gastroenterol. 2015;22(2):70-74.
- Singh A, Aggarwal M, Chadalavada P, et al. Natural history of gastrointestinal schwannomas. Endosc Int Open. 2022;10(6):E801-E808.
- Deprez PH, Moons LMG, OʼToole D, et al. Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. 2022;54(4):412-429.
Authors
Nadine Amaral, Filipe Taveira, Francisca Côrte-Real, Ana Rita Silva, Ana Catarina Rego, Nuno Paz
Gastroenterology Department, Hospital do Divino Espírito Santo de Ponta Delgada, Ponta Delgada, Portugal