Pesquisa
US Quiz of the Month – Dezembro 2023
Case Report
A 65-years-old female patient presented with hoarseness. Personal history includes a smoking habit (35 pack-years). Chest X-ray showed a pulmonary nodule. Chest computed tomography revealed a tumoral apical lesion of the right upper lobe, measuring 35x32x23 mm, in contact with the mediastinic pleura, arterial brachiocefalic trunk and subclavian vein (Fig.1). This lesion was not accessible by bronchoscopy.

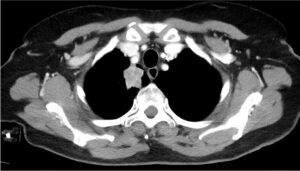
Figure 1. – Right upper lobe lung mass, showed on chest computed tomography.
The patient underwent a transesophagic endoscopic ultrasound-guided biopsy of pulmonary nodule, with 22G AcquireÒ needle (Fig.2).
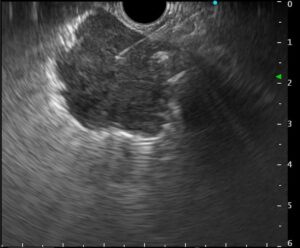
Figure 2 – Endoscopic ultrasound-guided biopsy of pulmonary nodule.
WHAT IS THE MOST LIKELY DIAGNOSIS?
Discussion:
After the endoscopic ultrasound-guided biopsy of pulmonary nodule, the patient underwent a right upper lobectomy with excision of paratracheal, subcarinal, and hilar lymph nodes. The histology of the specimen was consistent with lung adenocarcinoma displaying acinar, micro-papillary, and solid patterns, with visceral pleural invasion, with clear margins, measuring 32 mm. There was no angioinvasion. Due to pleural invasion and persistent pretracheal lymph node involvement, the decision was made to proceed with chemotherapy.
Lung neoplasia stands as one of the leading causes of both mortality and morbidity. Timely diagnosis is imperative, involving the acquisition of histological evidence. In the case of mediastinal lesions situated in the subcarinal, paraesophageal, aortopulmonary window, and para-aortic areas, fine-needle aspiration or fine-needle biopsy procedures are recommended, guided by either endoscopic or endobronchial ultrasound.1
Endoscopic ultrasound-guided fine-needle biopsy or aspiration can be an alternative when intraparenchymal lung masses are inaccessible through bronchoscopy or endobronchial ultrasound.2 This safety and effective technique offers a potential diagnostic approach to lung cancers in contact with esophagus.1
References
- Giri, S et al. Transesophageal endoscopic ultrasound-guided tissue acquisition of lung masses: a case series with systematic review and meta-analysis. Ann Gastroenterol. 36(2): 185-194, Mar-Apr 2023.
- Mangiavillano, B. et al. Transesophageal endoscopic ultrasound in the diagnosis of the lung masses: a multicenter experience with fine-needle aspiration and fine-needle biopsy needles. Eur J Gastroenterol Hepatol. 34(7):p757-762, July 2022.
Authors
Francisca Côrte-Real1, Nuno Nunes1, Diogo Bernardo Moura1, Maria Antónia Duarte1.
- Gastroenterology Department, Hospital do Divino Espírito Santo de Ponta Delgada, Ponta Delgada, Portugal.