Pesquisa
US Quiz of the Month – June 2019
CASE REPORT
A 65-year old female was referred to our Gastroenterology Department due to persistent upper abdominal pain and significant weight loss (20Kg) over the previous year. CT revealed a large retroperitoneal hypodense mass, in contiguity with the pancreatic body and tail, with encasement of the celiac trunk and superior mesenteric artery. Endoscopic ultrasonography (EUS) documented an extensive retroperitoneal hypoechoic lesion encasing the aorta, celiac trunk, common hepatic artery (Figure 1) and superior mesenteric artery (Figure 2), without vascular invasion (hyperechoic vascular wall interface was preserved), causing minimal compression of the pancreas.

Figure 1. Endoscopic ultrasonography (transduodenal view): retroperitoneal hypoechoic lesion encasing the common hepatic artery, causing minimal compression of the pancreas.

Figure 2. Endoscopic ultrasonography (transgastric view): retroperitoneal hypoechoic lesion encasing the superior mesenteric artery (AMS), without vascular invasion (hyperechoic vascular wall interface was preserved).
Transgastric EUS-guided FNB (22G, Acquire, Boston Scientific) of the retroperitoneal mass was performed, coursing anterior to the aorta between the celiac trunk and the superior mesenteric artery (Figure 3).

Figure 3. Transgastric EUS-guided FNB (22G, Acquire, Boston Scientific) of the retroperitoneal mass.
WHAT IS THE MOST LIKELY DIAGNOSIS?
DISCUSSION
Biopsy revealed spindle-shaped tumor cells and clusters of ganglion cells, with an eccentric large round vesicular nucleus and prominent macro nucleoli, consistent with ganglioneuroma (Figure 4).
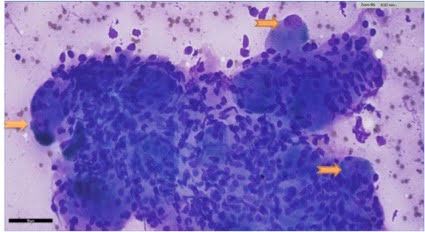
Figure 4. Cytology (Magnification: 400x; scale bar corresponds to 50 µm): Spindle-shaped tumor cells and clusters of ganglion cells, with an eccentric large round vesicular nucleus and prominent macro nucleoli (arrows).
The retroperitoneum can host a wide spectrum of pathologies, including a variety of rare benign tumours and malignant neoplasms.1 Tumours usually present late and cause symptoms or become palpable once they have reached a significant size.1 With the advent of EUS, gastroenterologists may be called upon to assist in the diagnosis and management of these lesions.
Some retroperitoneal tumours have specific patterns of growth and extension that aid narrowing the differential diagnosis.2 Some tumours grow and extend into spaces between pre-existing structures and surround vessels without invading the vessels walls. Ganglioneuromas and lymphomas typically present such pattern.2 Retroperitoneal metastatic carcinomas and leiomyosarcomas typically invade the vessels, causing thrombosis.2 Idiopathic retroperitoneal fibrosis, characterized by fibroinflammatory tissue surrounding the abdominal aorta, was also a valid alternative diagnosis in this setting.3
The reported incidence of ganglioneuroma is one per million population and the most common locations are the posterior mediastinum and the retroperitoneum.4 The diagnosis is challenging and is usually based on histopathological findings in surgical biopsies/specimens.4
REFERENCES
- Brennan C, Kajal D, Khalili K, et al. Solid malignant retroperitoneal masses – a pictorial review. Insights Imaging2014; 5(1):53-65.
- Nishino M, Hayakawa K, Minami M, et al. Primary retroperitoneal neoplasms: CT and MR imaging findings with anatomicand pathologic diagnostic clues.Radiographics2003; 23(1):45-57.
- Kermani TA, Crowson CS, Achenbach SJ, et al. Idiopathic retroperitoneal fibrosis:retrospective review of clinical presentation, treatmentand outcomes. Mayo Clin Proc2011; 86(4):297-303.
- Rha SE, Byun JY, Jung SE, et al. Neurogenic tumors in the abdomen: tumor types and imaging characteristics. Radiographics 2003;23:29–43.
AUTHORS
Miguel Bispo1, Susana Marques1, Ricardo Rio-Tinto1, Paulo Fidalgo1, Mireia Castillo-Martin2
- Gastroenterology Department, Champalimaud Foundation, Lisbon, Portugal.
- Pathology Department, Champalimaud Foundation, Lisbon, Portugal.